
All Global Research articles can be read in 51 languages by activating the Translate Website button below the author’s name (only available in desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Click the share button above to email/forward this article to your friends and colleagues. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Global Research Wants to Hear From You!
***
In this November 2023 presentation given in the Romanian Parliament, I provided evidence regarding the true efficacy of Covid-19 “vaccines”.
Other International Crisis Summit experts there revealed many details regarding the unprecedented deaths and injuries that follow these injections.
For my presentation, I set aside the monumental side effects, to evaluate the supposed purpose of the injections: to stop or reduce covid-19 infections. Here is the video of that presentation, as well as the same material in written format.

Click here to watch the video
The True “Efficacy” of COVID-19 “Vaccines”
Introduction
Covid-19 experimental genetic injections have been referred to as “safe and effective vaccines” though they do not satisfy that definition or those claims. They are physically not like any vaccine ever administered before.
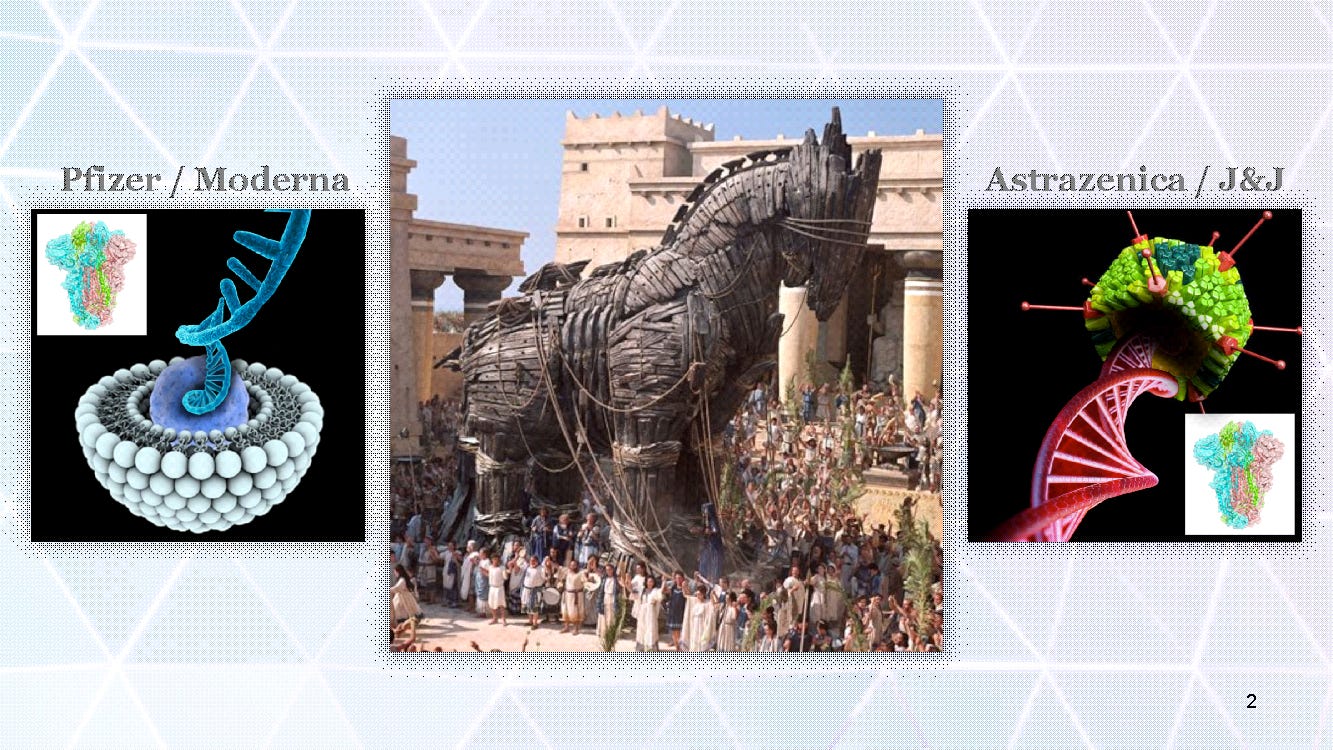
Pfizer / Moderna covid “vaccines” carry a payload of genetic mRNA for the spike protein in a special nanoparticle, while Astrazenica / Johnson & Johnson deliver full strand DNA in an adeno virus.
Not Safe, Not Effective
They do not block infection. They do not block transmission. They were predictably a failure and should not have been administered at all. The manufacturers’ clinical trials were inadequate, flawed, and in my opinion fraudulent. Efficacy claims to the public were deceptive.
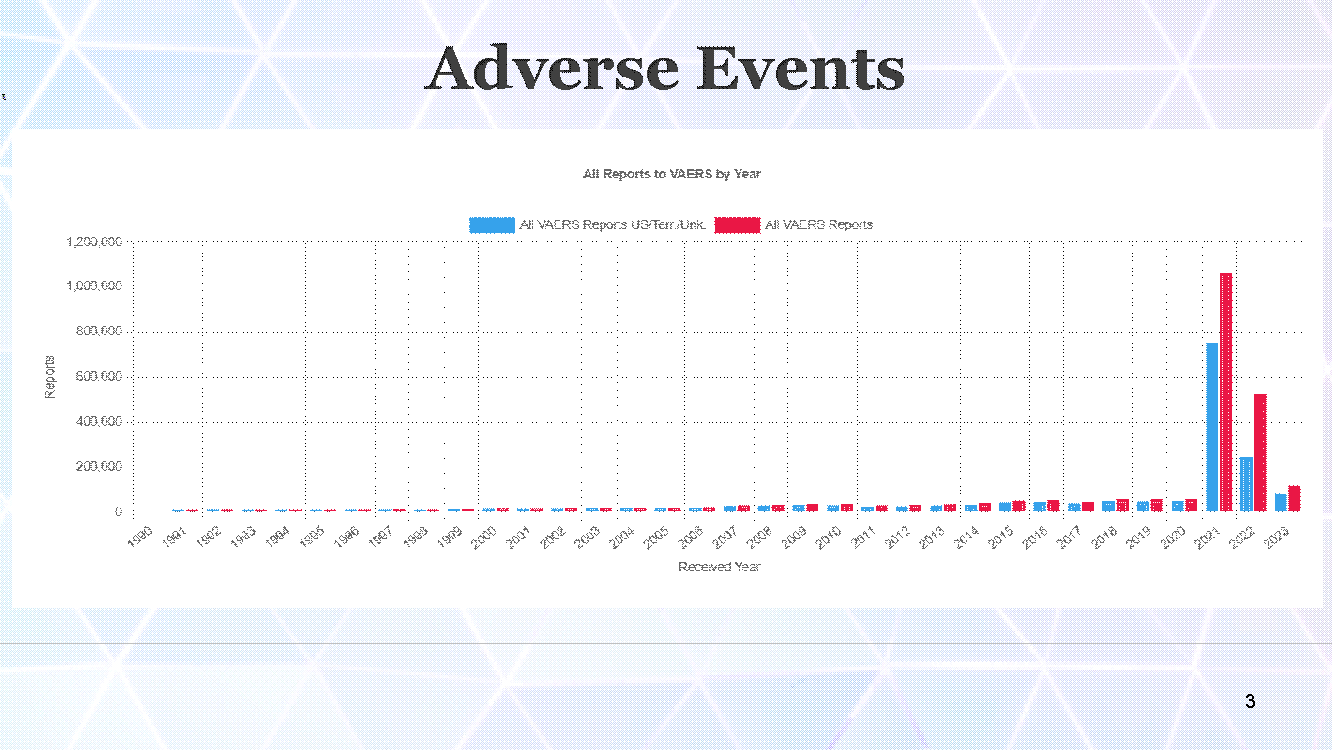
Real-world data clearly demonstrates that in addition to causing unprecedented adverse events …
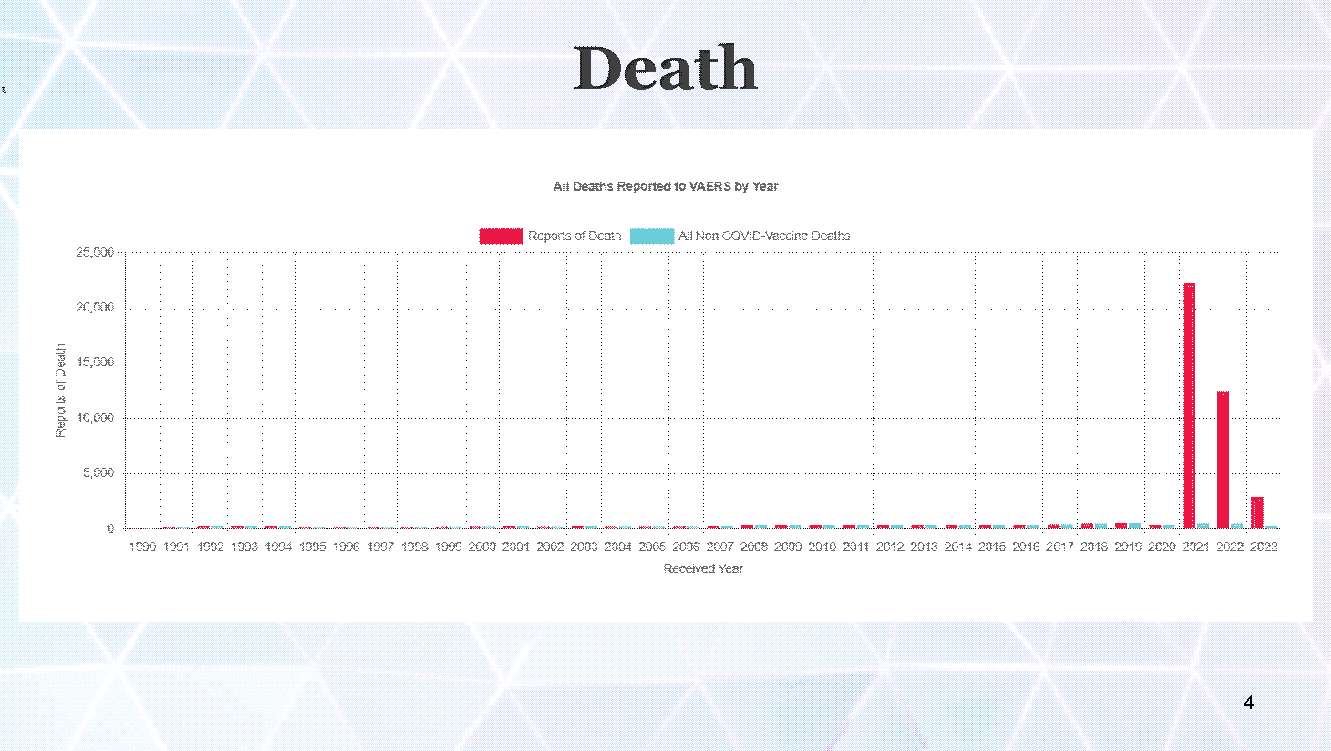
And death by multiple mechanisms…

These injections ultimately increase ones risk of covid-19 disease; with more injections rendering progressively higher risk of disease.
Predictable Failure and Persecution of Whistleblowers
Why, as early as 2020, before the covid injection campaigns started, did many doctors and scientists around the world, including myself, endure great professional and financial persecution, in the process of warning you against these injections? It’s because they were predictably harmful! Prior to the global experiment, the predicted efficacy of these injections was very poor.
There are many mechanisms of injury and death from the injections which my colleagues will describe to you, and I will gladly discuss during our interactions. These include general immune system dysfunctions that worsen all infectious diseases and cancers.
However, the subject of this article is specifically these injections’ impact on frequency or severity of covid-19 infections. Though as we note they fail to meet the definition of vaccines, we will describe their efficacy in terms of how effective are they at reducing coronavirus infections.
There efficacy was predictably bad. Here are a few of the reasons:
Antibody Dependent Enhancement
Click here to watch the video
Coronavirus Vaccines Caused Death and Illness in Prior Animal Trials
First, prior coronavirus vaccine research had revealed that antibodies induced through experiments can actually worsen outcomes rather than helping. When exposed to the actual disease, vaccinated laboratory animals often suffered worse illness and higher death rates than the unvaccinated control animals.
Second, these injections though labeled as “vaccines” were indeed genetic injections. Pfizer and Moderna covid-19 “vaccines” used messenger RNA technology. There have only ever been 385 human subjects in mRNA technology experiments prior to covid-19. These experiments demonstrated poor performance and high levels of adverse events with this technology.
Antibody Mediated Selection

Click here to watch the video
Third, vaccinating a population during a pandemic violates a fundamental principle of vaccinology, which is that one should never try to vaccinate the way out of a pandemic. The reason for this is that doing so places evolutionary pressure on the virus, and drives the evolution of one variant after another. This obstructs the natural path to herd immunity which normally would have ended the pandemic in a matter of a few months.
A fourth reason we predicted negative impact from these injections is the importance of the innate immune system and its development, especially for children. This is threatened by these injections.
So those are some of the reasons that many of us strongly predicted that these injections would have negative “efficacy”, that is, that they would make matters worse.
It is beyond naive to think that with big Pharma’s multi-billion dollar budget, their scientists who created these injections, could not foresee these same problems.
What evidence do we have of efficacy from the “vaccine” manufacturers’ own documents?
Pfizer’s initial two months of clinical trial data, which they used to apply to medical regulators for emergency use authorization; and the partial continuation of that clinical trial, to create their six month clinical trial report, had many flaws.
For instance: Two months for Emergency Use Authorization, and 6 months for the published trial, was far too little time to legitimately assess safety or efficacy. 10 years would be a usual minimum for a normal vaccine, never mind these genetic experimental “vaccines”.
The trial was not designed to assess transmission, or clinically relevant endpoints like hospitalization or transmission.
Large numbers of “vaccinated” subjects were just eliminated from the study, so their results were absent, with no explanation.
There was a failure to actively track and record the health status and adverse events of all trial participants.
The study was prematurely unblinded and many of the “unvaccinated” control groups were injected with the “vaccine”.
Unreliable and manipulatable PCR tests were used to diagnose “covid cases” without even reporting the cycle threshold used. This meant that “unvaccinated” subjects were diagnosed as having covid infections on very sketchy grounds; and “vaccinated” subjects similarly were diagnosed as not having covid, though they clearly had worse outcomes and more death. Considering the unreliability of the PCR as an endpoint measurement, they should have turned to all cause outcomes.
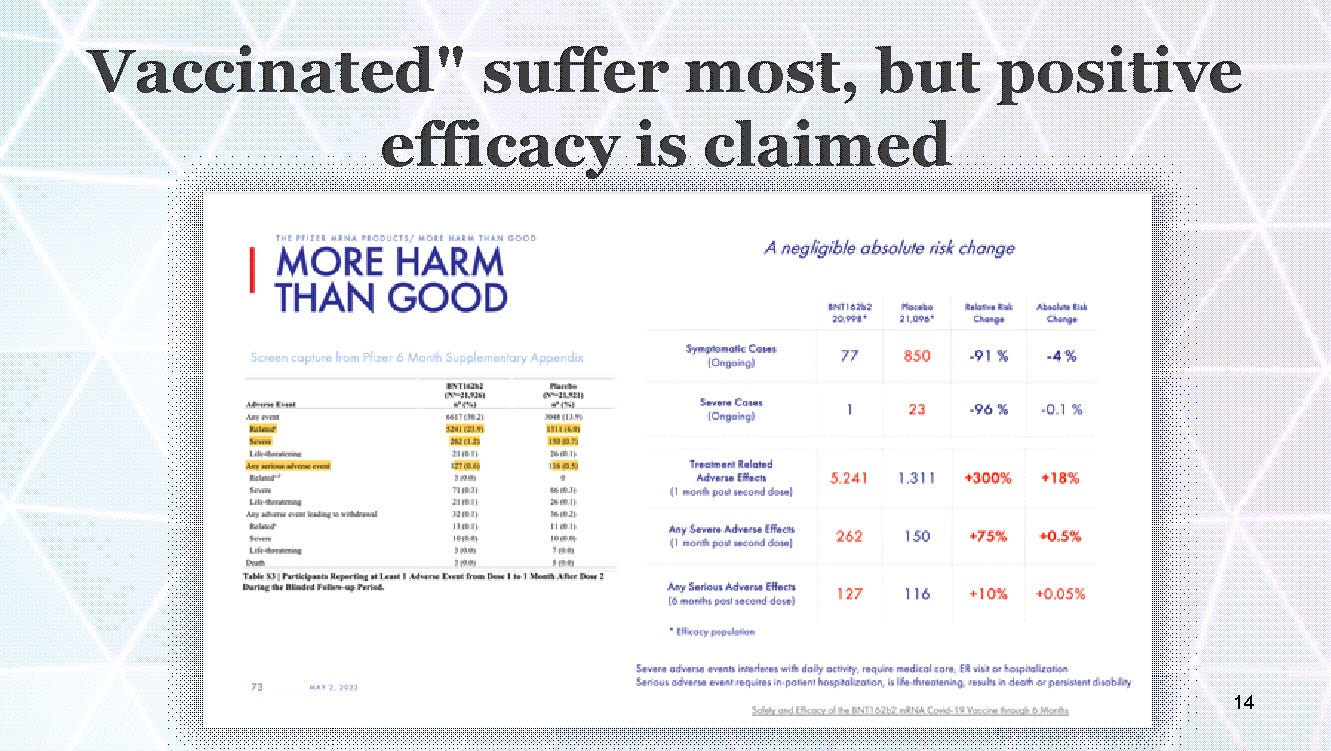
The “vaccinated” had much higher unsolicited adverse events (more sickness and disability), but the “vaccines” were still assigned as reducing symptomatic and severe cases of covid, while ignoring the reality that the “vaccinated” group suffered much worse disease and disability than the control group.
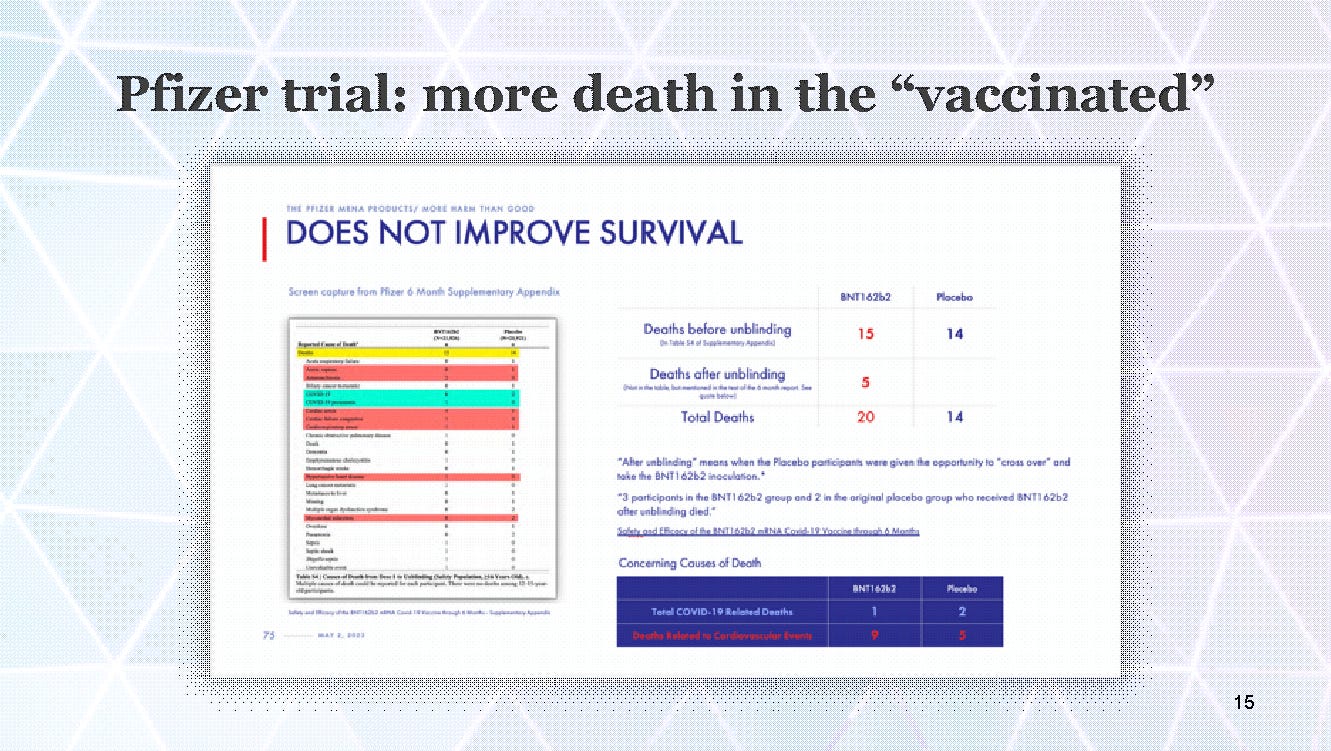
The Pfizer trial also had more death among the “vaccinated”.
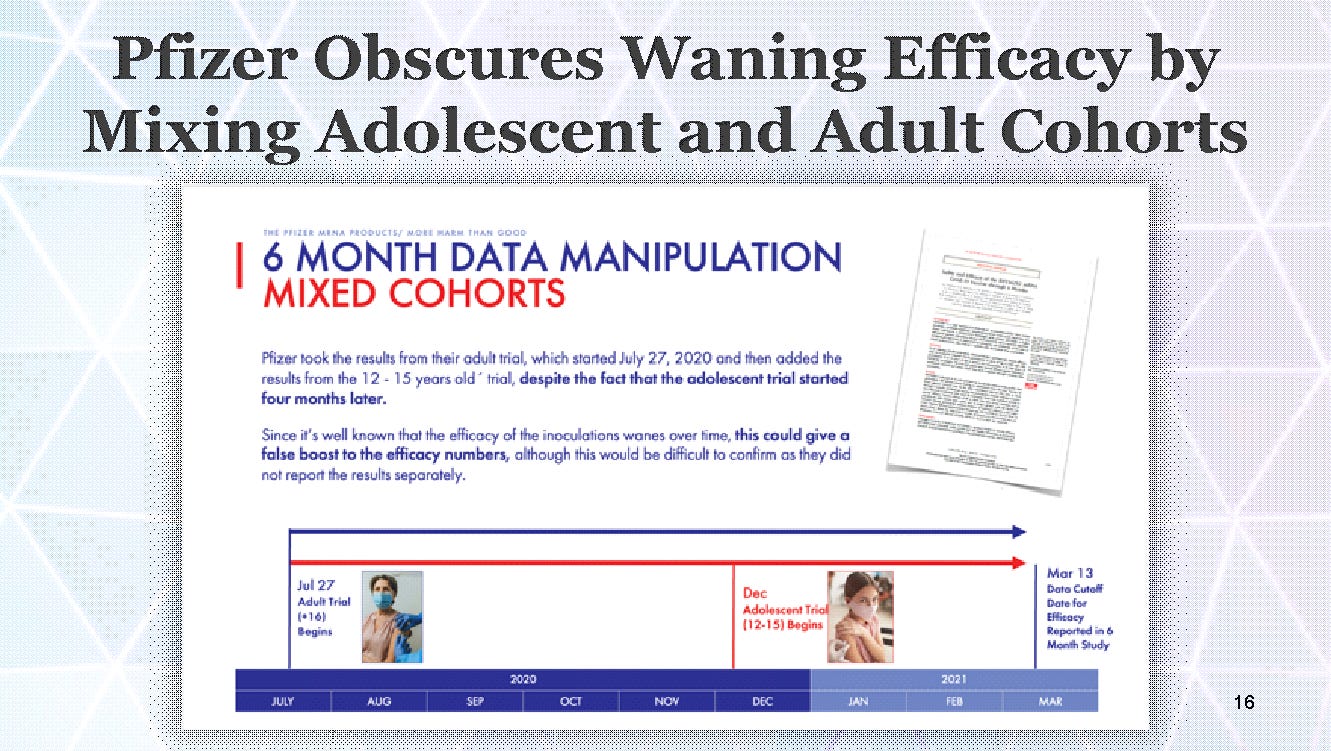
Pfizer may have covered up waning efficacy of the “vaccines” by combining the adolescent cohort group in with the adult group, even though the adolescent group started months later
Pfizer Wasn’t Alone in Performing Unacceptable Research…
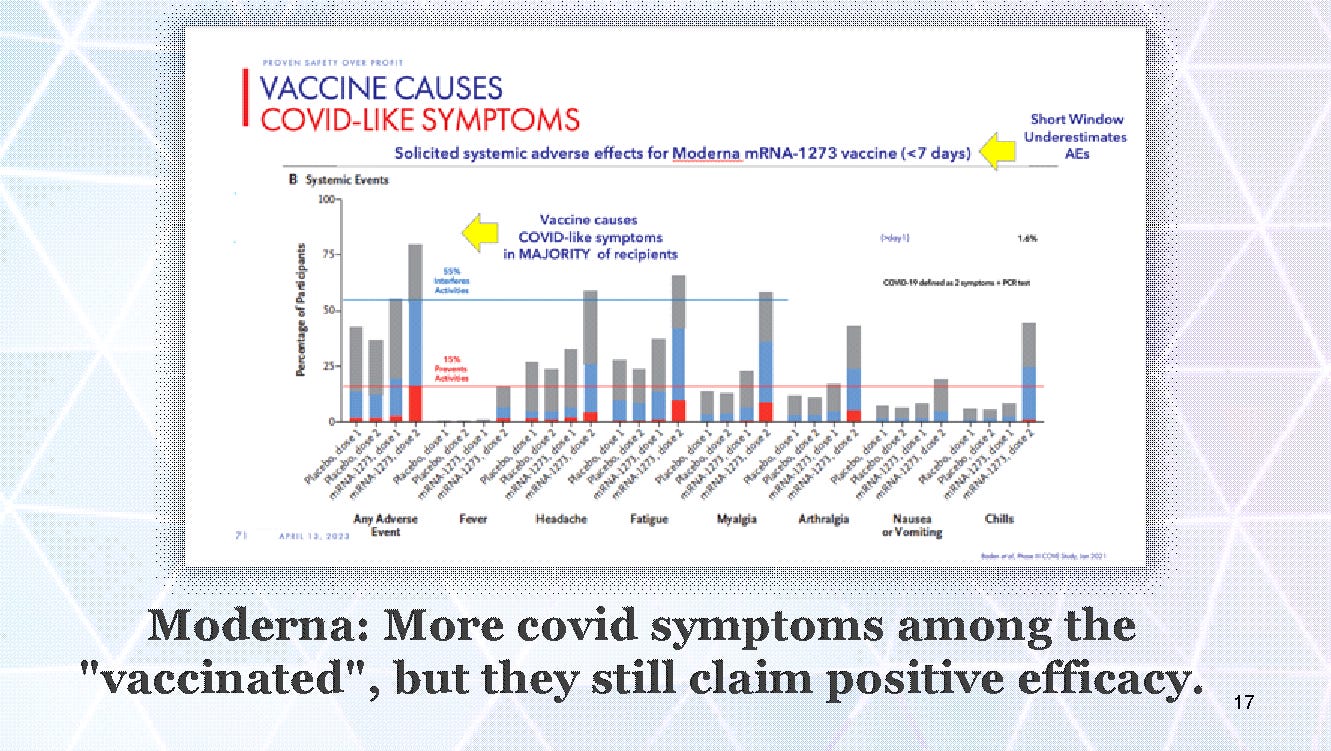
Moderna’s study showed increased “covid like symptoms” in the “vaccinated” group, but combined with a negative PCR (which is totally manipulatable, and the cycle threshold was not reported) they shuttled these patients to be counted as “not covid”, but instead something they labeled as “reactogenicity”. So despite the injected people having more and worse covid symptoms in the week after the injections, they were counted as not having covid, and like Pfizer, Moderna ultimately reported that the “vaccines” reduced covid infections.
With all these tricks in play, the manufacturers created a relative risk reduction claim of 95%, when the reality was likely much lower or even negative.
Notice here we are discussing “relative risk reduction”. This is not normal.
Reporting relative risk reduction is deceptive and unethical.
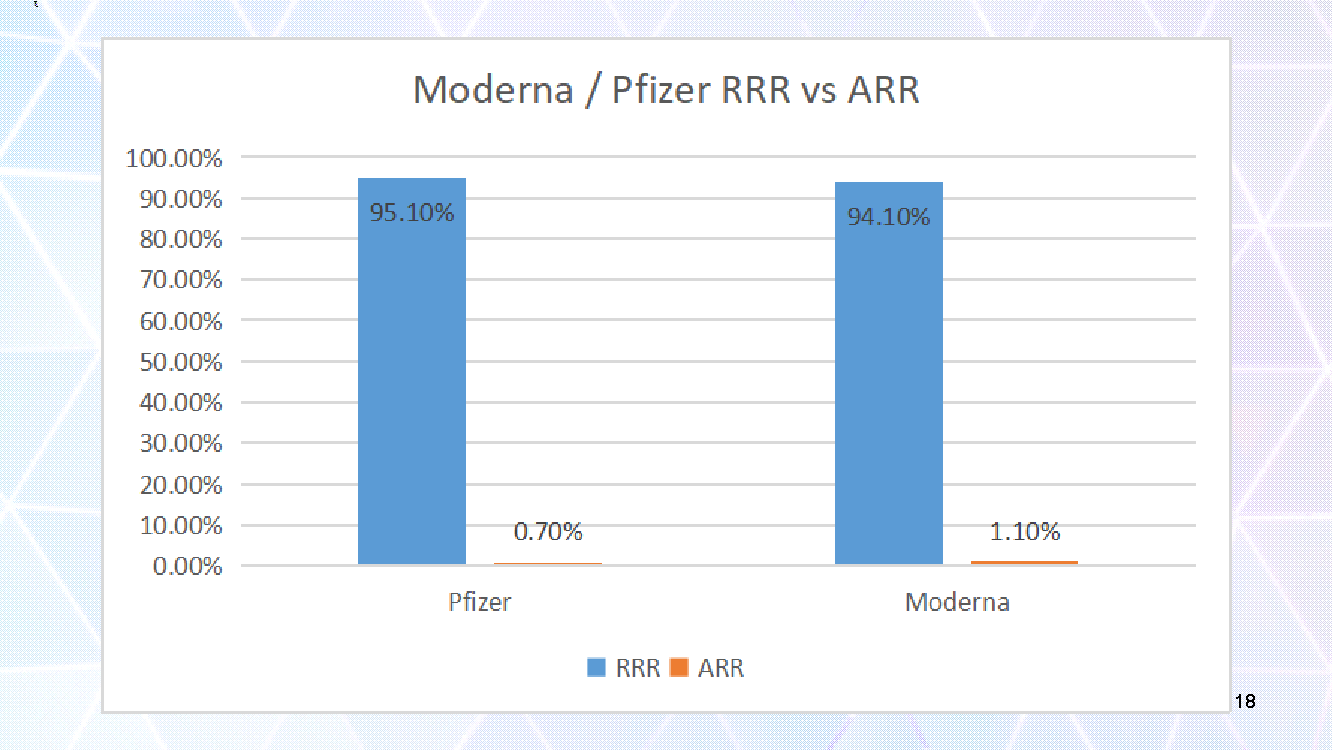
To make sound decisions about our health, we must be quoted absolute risk reduction. When Pfizer claimed their injections reduced the risk of covid disease by 95.1%, this actually meant it reduced the risk of covid disease by 0.7%.
The risk of covid disease was already very low without the “vaccine”, so a 95% RRR is a very small actual reduction in risk, or ARR. Moderna similarly claimed to reduce the risk of covid infection by 94.1% in their studies, but that was really just an absolute risk reduction of 1.1%.
Considering the many flaws, omissions, and deceptive practices in the studies, like the ones we just discussed, the true absolute risk reduction for covid disease was possibly even less than the reported 0.7% and 1.1% ARR.
It may have been negative. We will find out more with the real world data to follow.
These trials were not designed to assess transmission, or clinically relevant endpoints like hospitalization or death. The absolute harms clearly outweighed the absolute benefits for Pfizer’s 6 month data. People were coerced into experimental and dangerous injections that at most offered a sliver of benefit for reducing covid-19 disease, while increasing their total risk of harm.
How did these so-called “vaccines” perform once they were imposed on the public?
In short: poorly, and it was actively covered up by governments and medical regulators.
Governments reported some evidence that supported “vaccine” effectiveness, but these claims were doubtful because of a range of serious inconsistencies and anomalies, including counting people as “unvaccinated” until two or three weeks after their injections, so for instance an infection up to two weeks after injection was counted as an infection in an unvaccinated person.
People were considered “injected but not vaccinated” which is farcical.
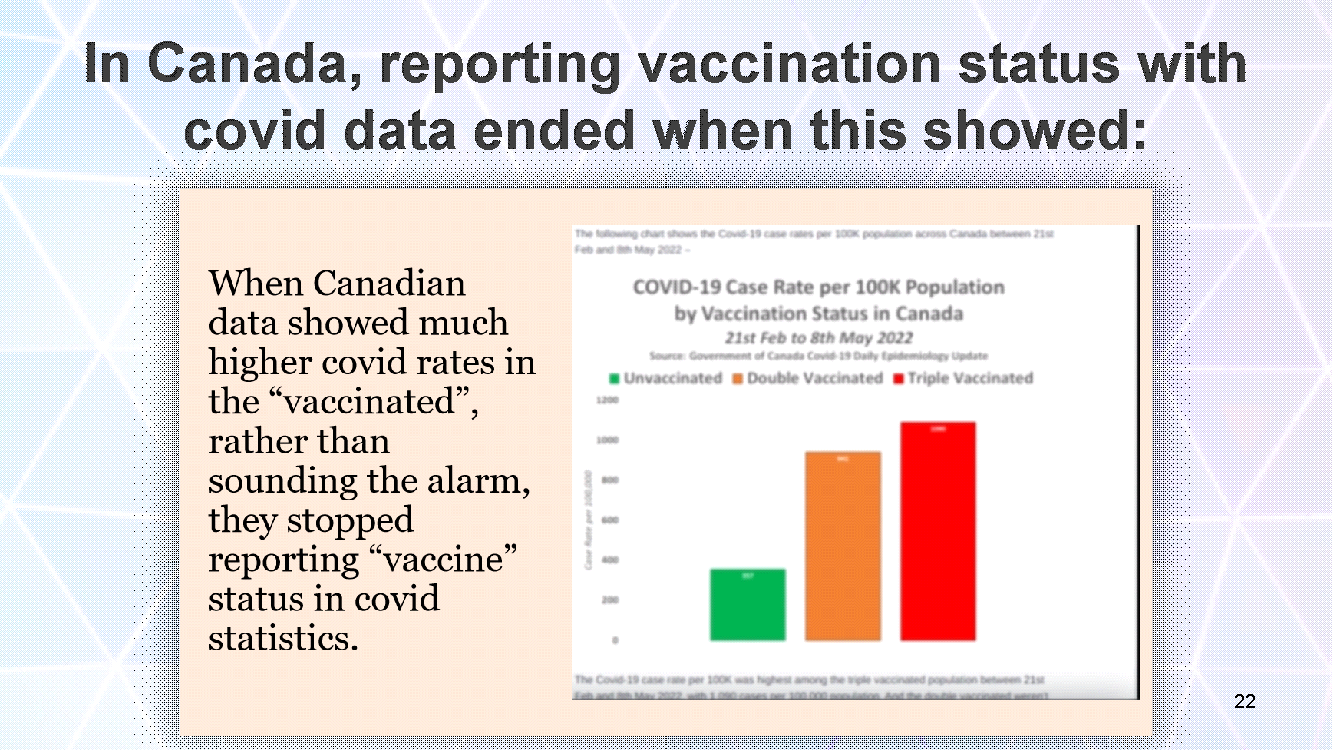
When government covid data showed infection rates highest in the most “vaccinated”, and lowest in the “unvaccinated”; rather than halt the injections and raise alarms, Canada’s governments stopped reporting “vaccination” status with the data. People were then blindfolded from seeing that it was predominantly “vaccinated” people suffering with covid-19 disease.
For example, by May 2022, Canadian data showed dramatically higher covid infection rates among the “vaccinated” than the unvaccinated, and even higher for triply injected person. Rather than responding in the best interest of the people, the government stopped reporting “vaccination” status with the covid statistics; then the public could no longer see what was happening.
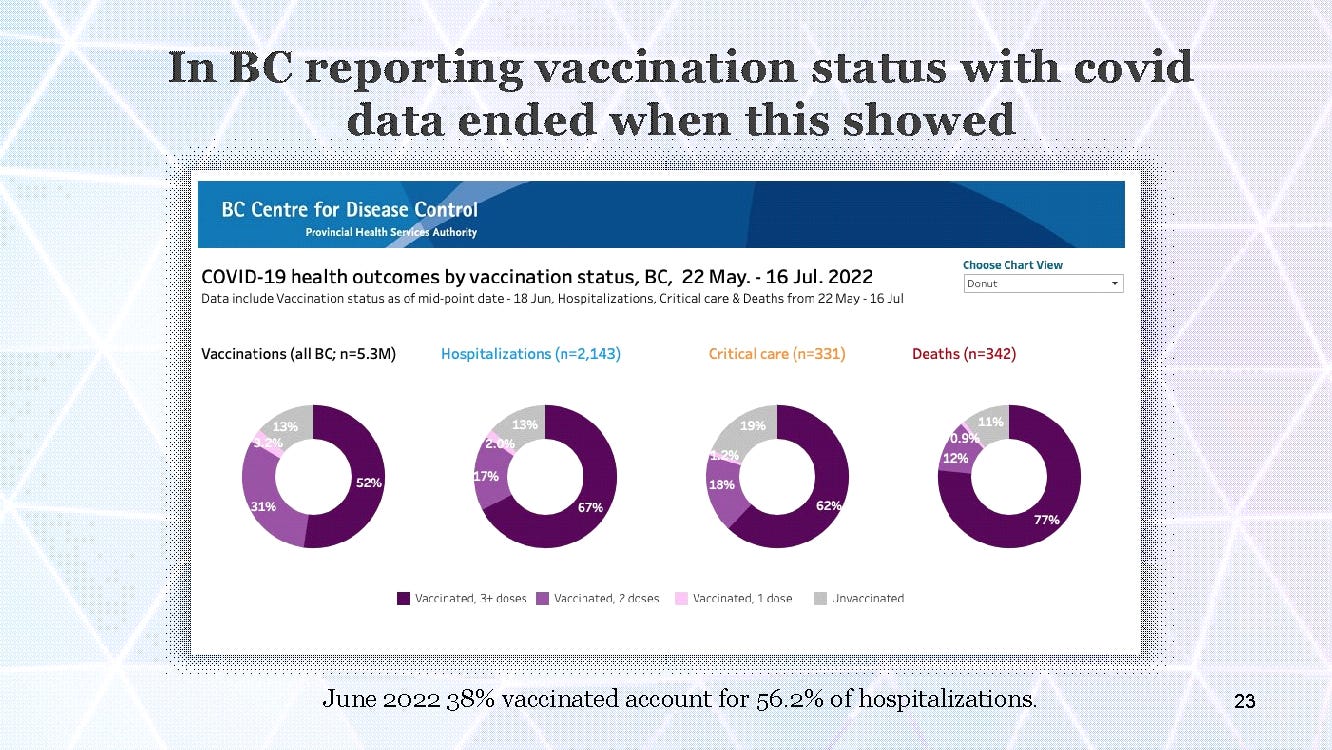
Here’s one example of provinces doing the same thing. This is from British Columbia. Negative efficacy became obvious by the summer of 2022. The BC government responded by ending the reasonable practice of reporting “vaccination” status with covid data.
Other provinces did the same.
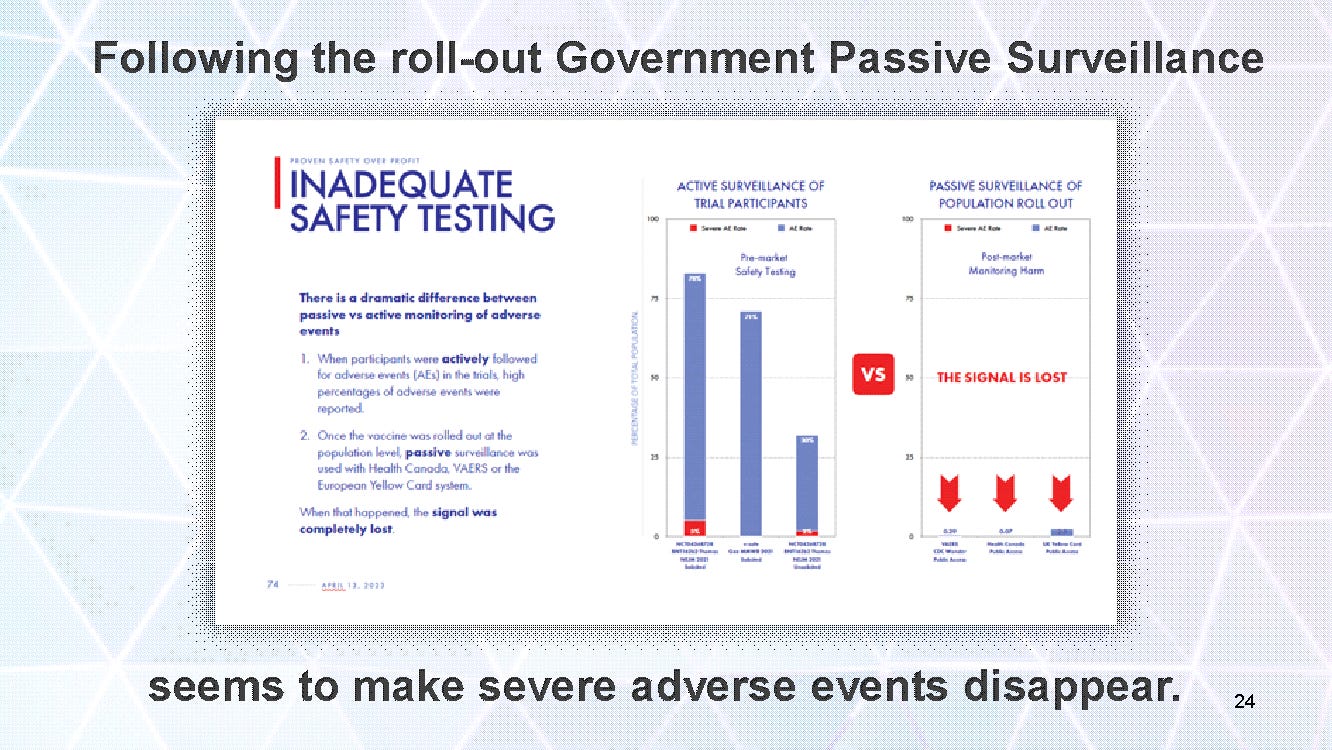
There is a severe difference between active surveillance in clinical trials and passive government surveillance used following the roll out. Passive surveillance systems seemed to make adverse events disappear.

In Canada, only physicians could report adverse events, patients could not.
The process was laborious, and doctors who tried to report adverse events, had their reports rejected, and they were investigated, disciplined, and often stripped of their licenses to practice medicine.
For example consider Dr Patrick Phillips of Ontario Canada, who maintained ethical and scientific integrity throughout the pandemic, and was unlawfully persecuted by the medical licensing body, the CPSO, and stripped of his career and income. Every adverse event he reported was rejected, and the CPSO responded to each of his attempted reports by launching another complaint against him, despite there being no patient complaints.
This is highly irregular.
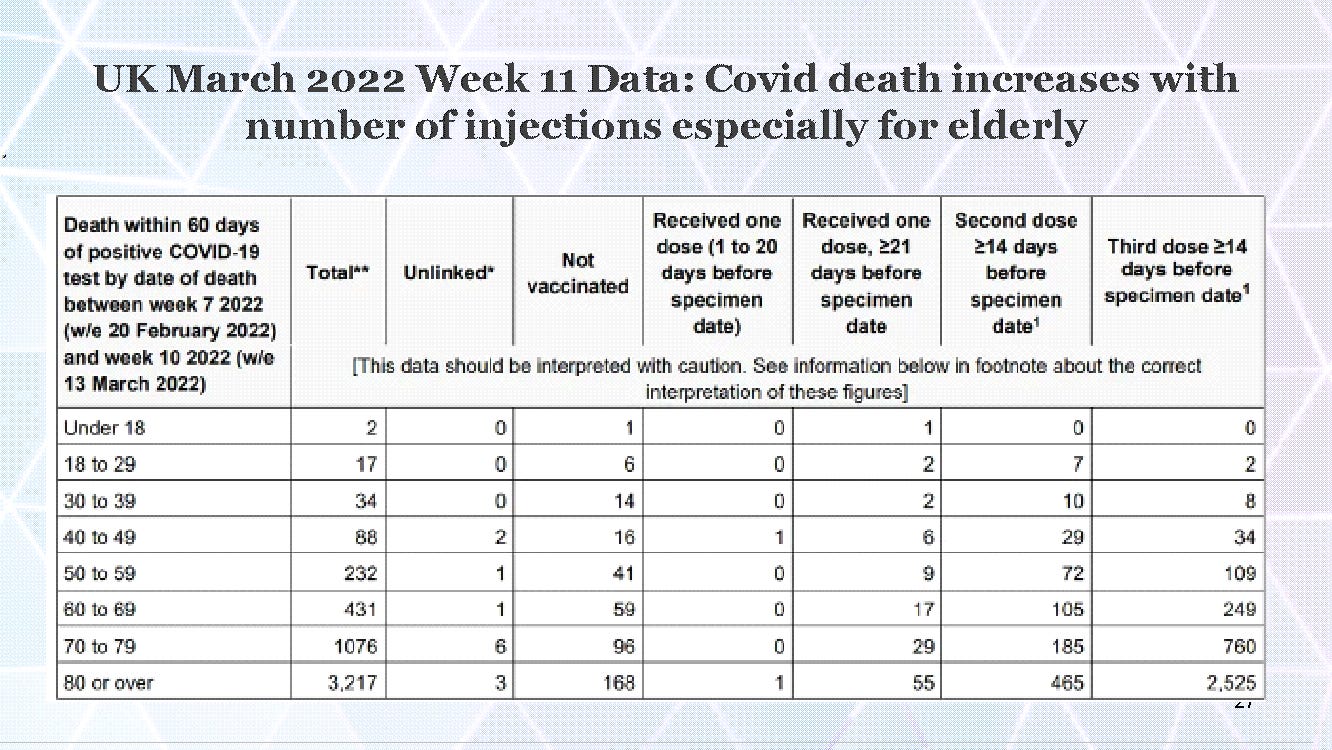
In the UK, by week 11 of the injection campaign in March 2022, government data showed overall increased covid-19 infections and deaths among the “vaccinated” compared to the “unvaccinated.” Scientists and doctors who showed negative effects of the “vaccines” were banned from publication and ousted from professional positions. Despite that, many studies contained data that did demonstrate negative efficacy.
A UK study of covid “vaccine” and disease statistics in June 2022, involving more than 9 million participants and comparing data for differing Body Mass Indexes, found (I quote) “Surprisingly, we observed a higher risk of test positivity after vaccination with one or two doses across all BMI groups, which is contrary to evidence reported by the UK Office of National Statistics.
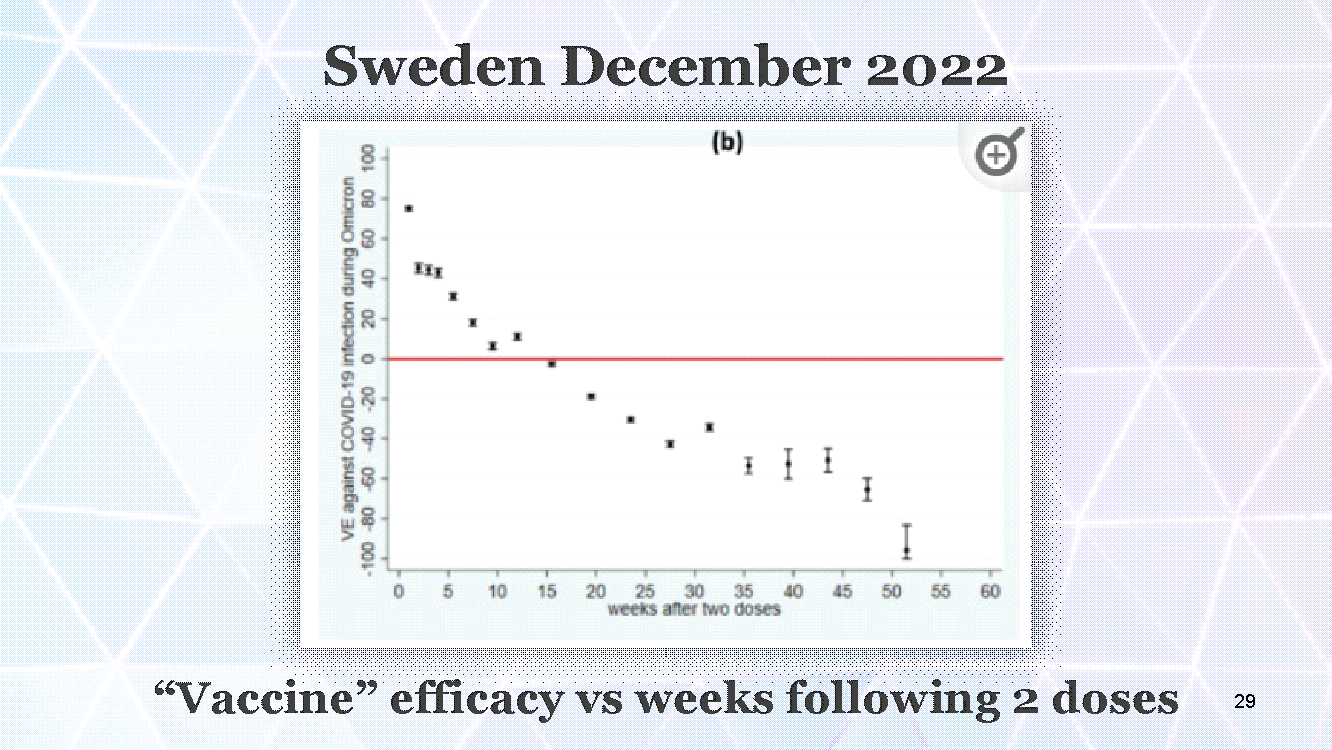
Here are some results from Sweden, December 2022, from a study titled: Effectiveness of COVID-19 “Vaccines” over 13 Months Covering the Period of the Emergence of the Omicron Variant in the Swedish Population.
This involved data from 9,153,456 Swedes. The researchers reported conflict of interest and conclusion that differed from the data, but regarding “vaccine” efficacy, they found “limited protection against Omicron infection (dropped to 43% by week four and no protection by week 14)” and by week 50 post injection “vaccine” efficacy dropped to nearly negative 100%, meaning it doubled the persons’ risk of covid infection.
Our data showed negative “vaccine” efficacy against Omicron infection from week 14, indicating that “vaccinated” individuals experienced a higher risk of infection than those unvaccinated.”
In Germany, in the fall of 2022, a covid outbreak occurred at an Ophthalmology conference. Every single person known to be infected was “vaccinated”.
The Cleveland Clinic in the USA employs more than fifty thousand persons.
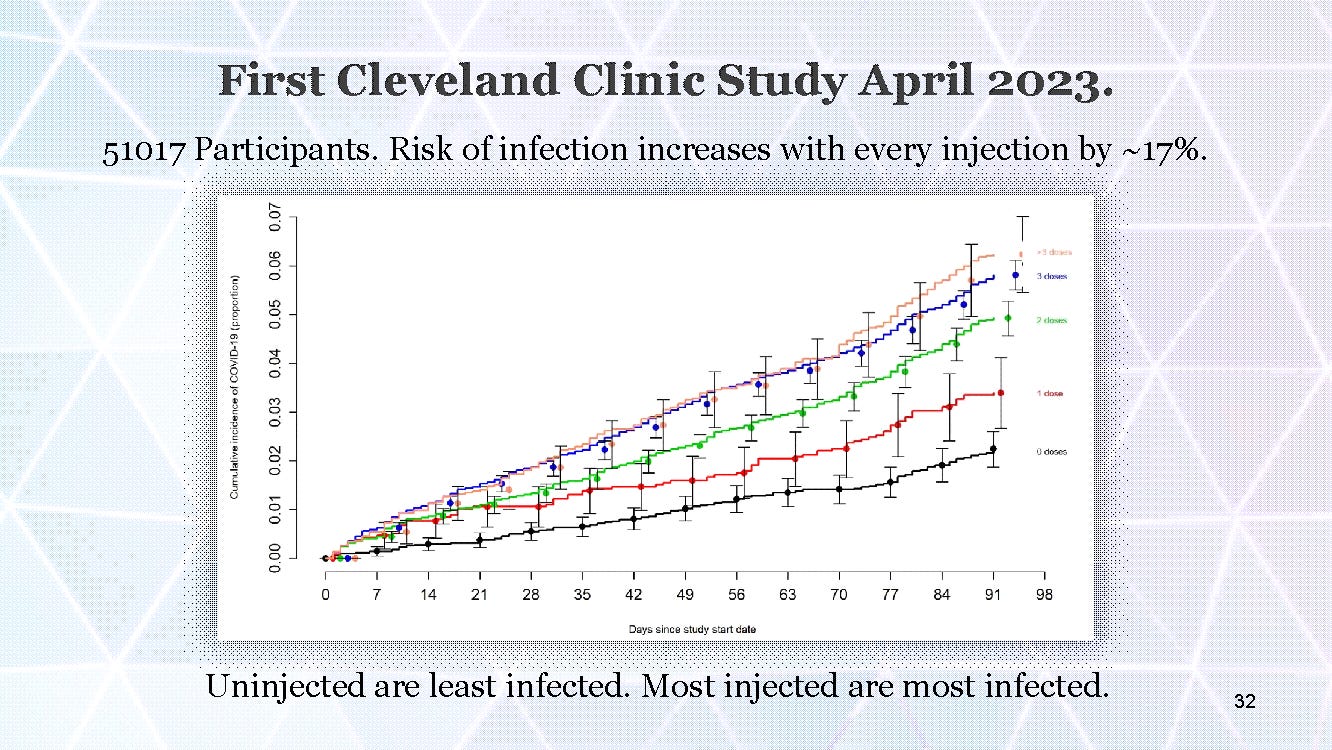
This study published in April 2023, involved 51,017 employees and clearly demonstrated negative efficacy of the “vaccines”, with the lowest infection rate in the “unvaccinated” and highest rates in the most injected. You can literally see how each injection increased the risk of infection by about 17%.
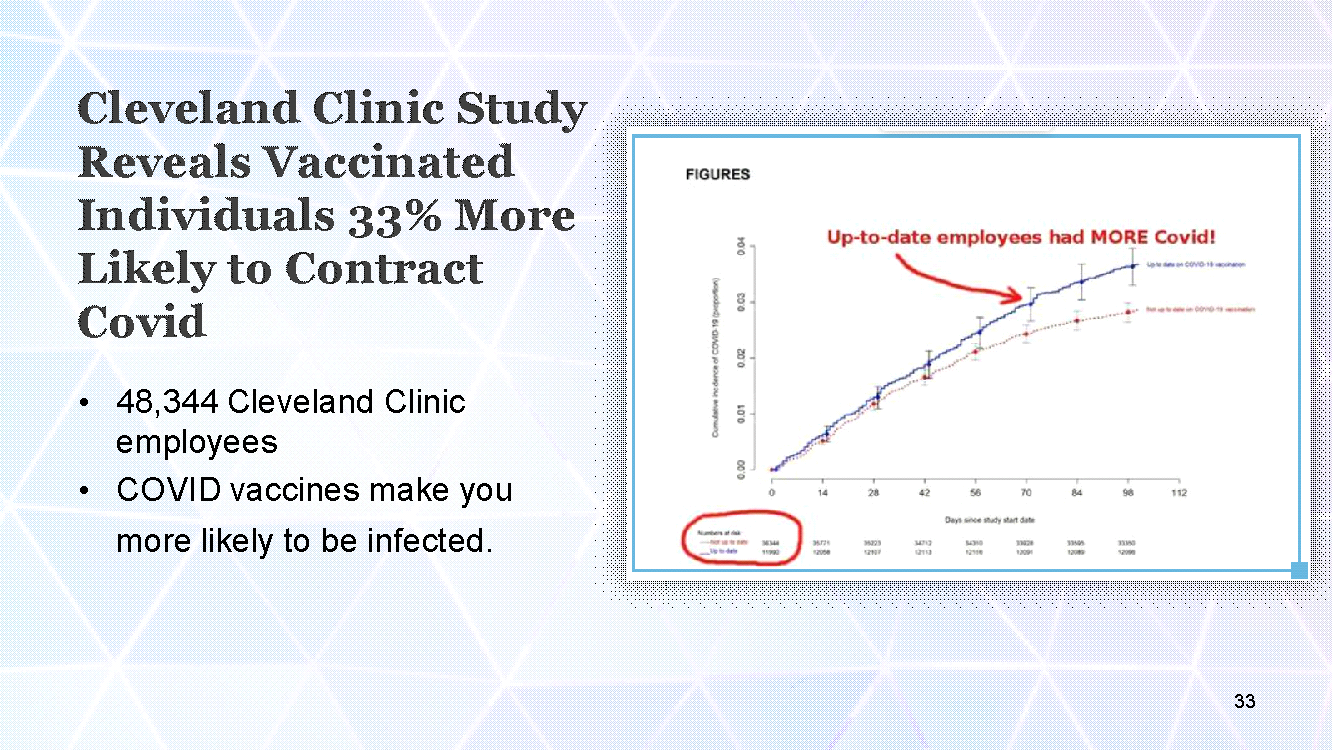
A second Cleveland Clinic study published in June 2023, demonstrated lowest infection rates in person “not up-to-date” on the “vaccines”, and highest rates in person “up-to-date”.
The researchers noted: “It is now well-known that SARS-CoV-2 infection provides more robust protection than “vaccination”. To say the least!
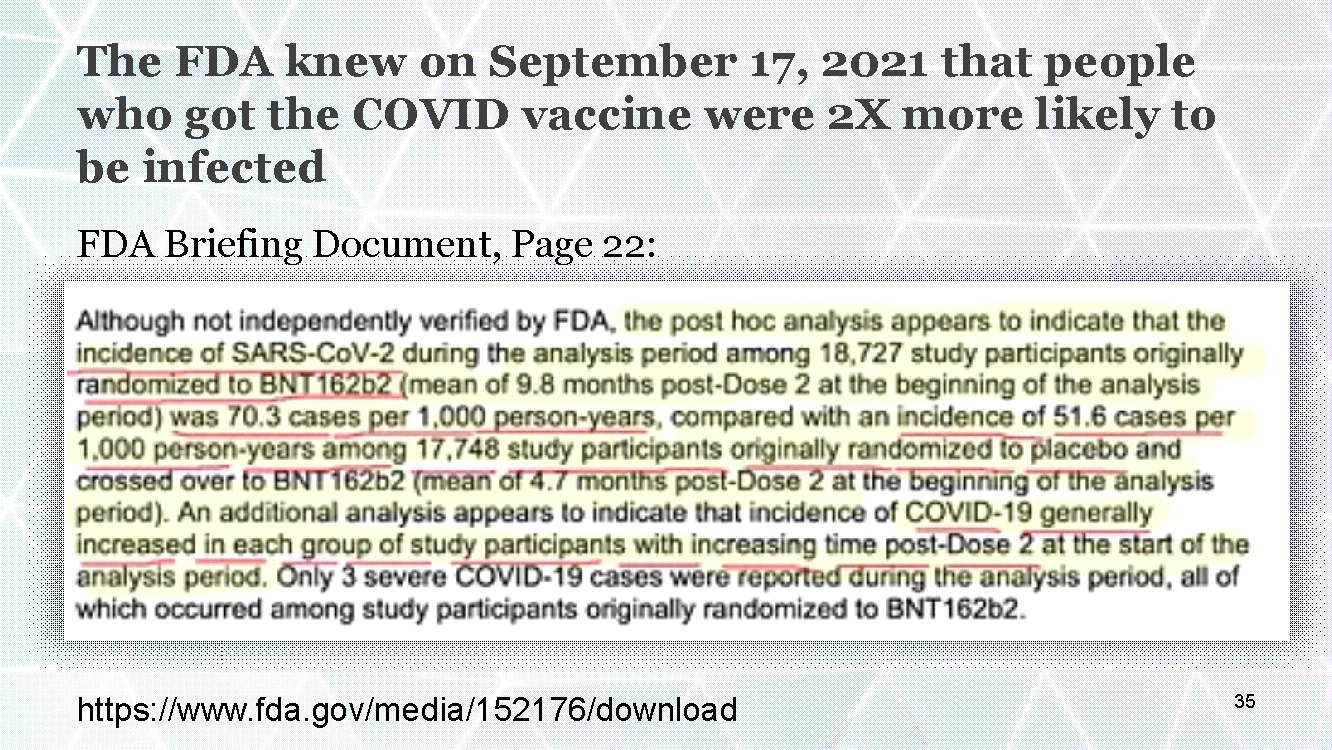
The USA FDA knew on September 17, 2021 that people injected with the Pfizer covid “vaccine” had double the risk of covid infection than the “unvaccinated”. This is from the Vaccines and Related Biological Products Advisory Committee Meeting September 17, 2021 FDA Briefing Document.
This document reported a covid-19 infection rate in the “vaccine” group of 70.3 cases per 1000 people, but only 51.6 cases per 1000 people who were originally in the control group and later “crossed over” and injected. It is safe to assume that they would have experienced an even lower infection rate had they not been injected at all.
It is scientifically deceptive and unethical to inject control subjects when they were clearly better off in terms of covid disease, adverse events, and death; but it did serve to reduce the magnitude of the negative efficacy that was demonstrated.
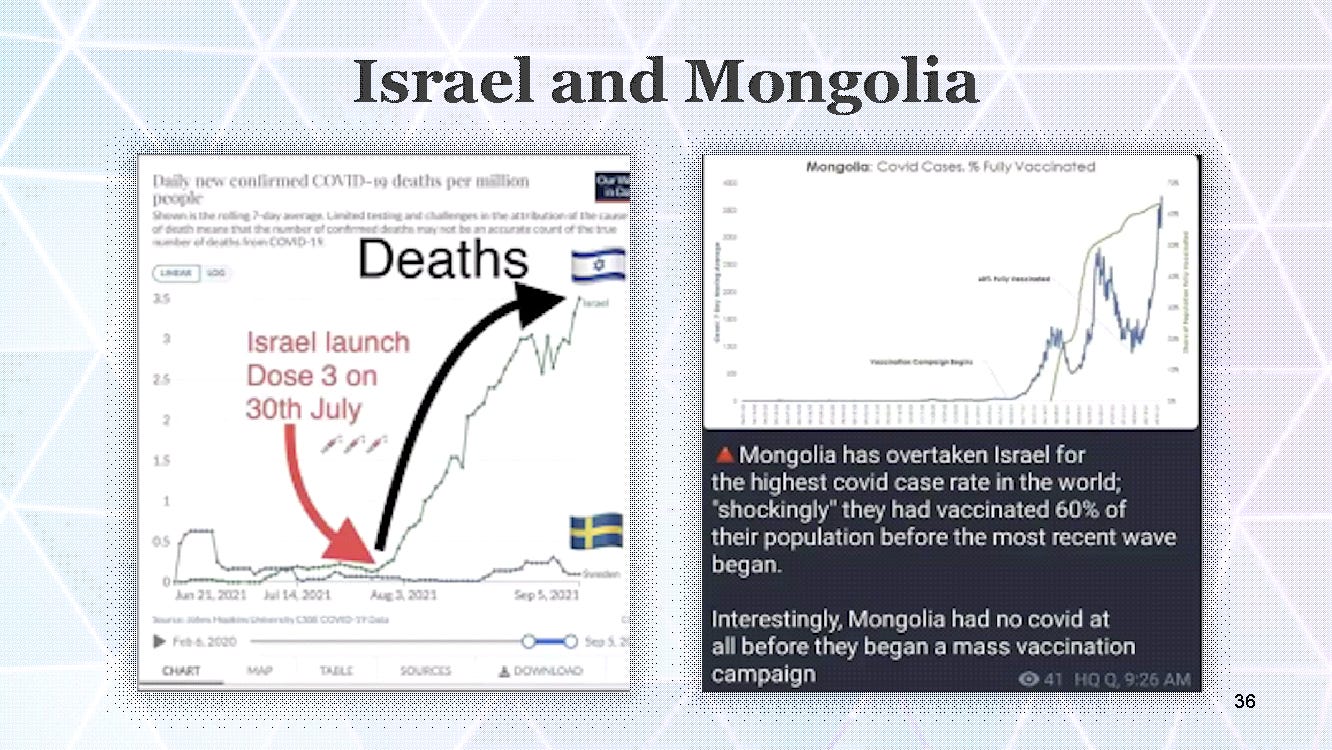
Israel launched their third dose on July 30, 2021 and deaths skyrocketed. In Mongolia covid infections were approximately zero until they launched their injection campaign in February 2021. Then infection rates soared.
The Amish:
Here’s another real world indication of the negative effects of the coerced and misrepresented covid-19 genetic injection “vaccines”, and the rest of the unscientific and unethical covid agenda.
The Amish did not participate in any of the covid agenda. They did not mask, social distance, close their schools, churches or businesses. They did not invite nor submit to the injection campaigns.
Amish people over 60 years old had a 23 times lower Infection Fatality Rate than the rest of the country.
For all age groups combined, their infection fatality rate from COVID was at least 90 times lower than the surrounding community.
The failure of the experimental genetic injections to perform as “vaccines” was predictable before they were launched. The manufacturers own studies were flawed, inadequate and riddled with efforts to obfuscate safety and dramatize benefit.
Relative risk reduction numbers presented to the public were deceptive. Real world evidence shows that in addition to the dramatic adverse events and deaths caused by these injections, they are complete failures with negative efficacy.
Covid-19 so-called “Vaccines” prolonged the pandemic, and increase individuals’ risk of covid-19 disease.
What should be done?
*
Note to readers: Please click the share button above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Sources
ADE References:
All images in this article are from the author
Comment on Global Research Articles on our Facebook page
Become a Member of Global Research
Source link