

Despite dozens of high quality trials, mechanistic studies, and widespread generic availability, there remains great resistance to oral statins to reduce the risk of athersclerotic cardiovascular risk (myocardial infarction, stroke, need for revascularization, and cardiovascular death). Alter AI assisted with this interesting paper from Japan.
The study “Measuring Public Preferences for Statin Therapy Using the Smallest Worthwhile Difference” (JAMA Internal Medicine, published online February 16, 2026) by Luo et al., explored how laypeople in the United States and Japan evaluate the benefits and burdens of statin therapy for primary prevention of atherosclerotic cardiovascular disease (ASCVD). Although clinical guidelines strongly recommend statins to reduce cardiovascular risk, these guidelines are based on expert judgment, whereas patients’ own preferences and thresholds for perceiving benefit remain poorly understood. The investigators applied an explicit decision-making metric—the Smallest Worthwhile Difference (SWD)—defined as the minimum absolute risk reduction in ASCVD events that individuals consider sufficient to justify long-term statin use.
Methods
Online surveys were administered to adults aged 40 to 75 years with no prior statin use. The samples—254 U.S. respondents and 297 Japanese respondents—were recruited through research panels using stratified sampling to approximate national demographics. Participants were educated about statin benefits and side effects, completed comprehension checks, and then answered iterative trade‑off questions using graphical displays. Each person reported the absolute risk reduction they would require to consider statin therapy worthwhile under three baseline 10‑year ASCVD risk scenarios: 2%, 10%, and 20%. The usual threshold for a doctor to recommend a statin is a 10-year actuarial risk of 10%. Most patients with 20% risk have already manifested atherosclerosis. Actual statin efficacy was provided as approximately a 25% relative risk reduction per 38.6 mg/dL decrease in LDL cholesterol (roughly a 2–3% absolute reduction) over two years.
.
Luo Y, Kawakami H, Funada S, et al. Measuring Public Preferences for Statin Therapy Using the Smallest Worthwhile Difference. JAMA Intern Med. Published online February 16, 2026. doi:10.1001/jamainternmed.2025.7958
.
Findings
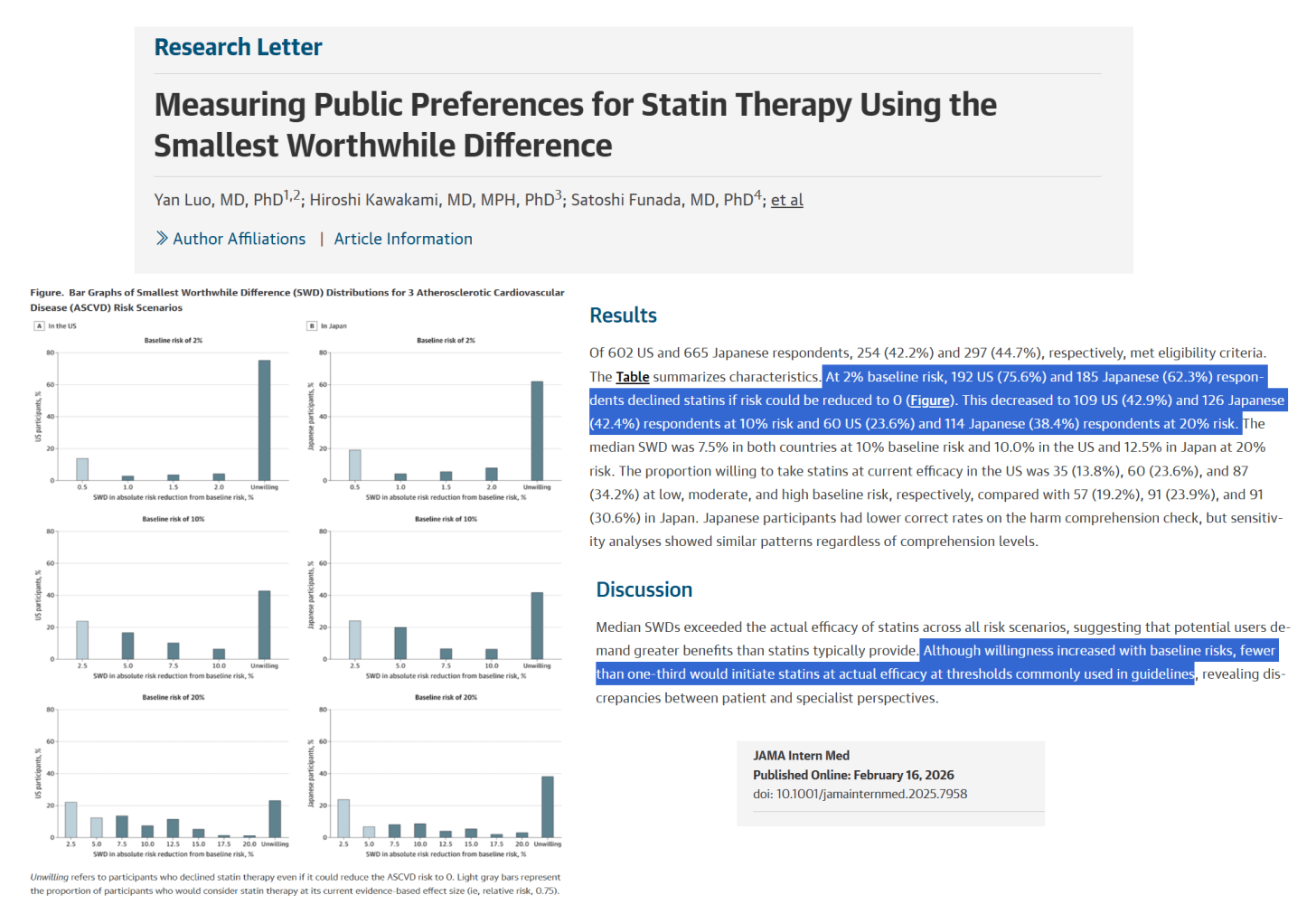
At a 2% baseline risk, 75.6% of U.S. and 62.3% of Japanese participants refused statins even if the drug completely eliminated ASCVD risk, showing strong reluctance toward preventive medication at low risk which is appropriate. Willingness increased modestly as baseline risk rose: at 10% risk, refusals dropped to 42.9% (U.S.) and 42.4% (Japan); at 20% risk, to 23.6% (U.S.) and 38.4% (Japan).
The median SWD—the required absolute risk reduction—was 7.5% in both countries at 10% baseline risk and 10.0% (U.S.) versus 12.5% (Japan) at 20% risk. This means the public expects a 75% relative risk reduction with statins over two years (baseline risk 10%). These thresholds substantially exceed the true benefit of statins, meaning that most respondents demanded a ten‑fold greater effect than the drug can deliver. Accordingly, only a minority would accept statins at real‑world efficacy: in the U.S., 13.8% at 2% risk, 23.6% at 10% risk, and 34.2% at 20% risk; in Japan, 19.2%, 23.9%, and 30.6%, respectively. Japanese respondents scored lower on comprehension of adverse effects, yet sensitivity testing confirmed similar overall patterns.
Interpretation
Across both nations, people required substantially larger benefits than statins provide before considering therapy worthwhile. This disconnect suggests that the public values absolute benefit magnitude more than professional guideline writers assume. The similarity between countries, despite differing health systems and ASCVD prevalence, indicates a shared human tendency to weigh small preventive benefits against financial, practical, and perceived safety burdens.
Implications
The results highlight a persistent gap between patient expectations and what medication can deliver. Integrating SWD analysis into guideline development could enable more transparent, value‑based risk thresholds and improve shared decision‑making. For clinicians, expressing benefits in absolute rather than relative terms may align expectations and foster trust.
Conclusion
Most adults in both the U.S. and Japan believe statin benefits are insufficient to justify therapy for primary prevention. There is a mismatch between population expectations and real benefits of statins. The public wants more risk reduction than statins can deliver.
*
Click the share button below to email/forward this article. Follow us on Instagram and X and subscribe to our Telegram Channel. Feel free to repost Global Research articles with proper attribution.
Source
Luo Y, Kawakami H, Funada S, et al. Measuring Public Preferences for Statin Therapy Using the Smallest Worthwhile Difference. JAMA Internal Medicine. Published online February 16, 2026. doi: 10.1001/jamainternmed.2025.7958
Global Research is a reader-funded media. We do not accept any funding from corporations or governments. Help us stay afloat. Click the image below to make a one-time or recurring donation.


